A Public Symposium presented by
the Rinbutsuken Institute for Engaged Buddhism
the Sophia University Institute of Grief Care
the Tokyo Jikei Medical University Palliative Care Center
November 4, 2017
Tokyo Jikei School of Medicine, Tokyo
Introduction
The practice of Buddhist based mindfulness meditation is now sweeping the world. Entering various secular fields like business, medicine, and even sports, mindfulness practice has helped people to reduce work related stress, be more efficient and focused in their endeavors, and find a pathway to inner peace. There are, however, critics of this movement—including the Buddhists that helped spawn it—who point out that mindfulness meditation (samadhi) in and of itself is not sufficient for true transformation and that isolating it from the ethics (sila) and a deeper understanding of the roots of ignorance (panna) can distort the practice in unfortunate ways. Furthermore, as wonderfully simple as mindfulness may seem, it is usually not a practice that is accessible for the deeply traumatized, such as those experiencing suicidal depression, recovering from a natural disaster or traumatic event, or dealing with the grief of a lost loved one. To become intimate with such people, and to be able to guide them to a place of stability from which an intensive mindfulness practice could be of help, requires a type of caregiver or “guide” who is in fact highly developed in all three of these facets of mindfulness, ethics, and the accompanying wisdom and resilience it requires to engage deeply in suffering.
On November 4, 2017, these two issues—understanding mindfulness in a more holistic manner and applying this holistic approach to caregiving—were grappled with at a public symposium jointly hosted by the Rinbutsuken Institute for Engaged Buddhism, the Catholic based Sophia University Institute of Grief Care, and the Tokyo Jikei Medical University Palliative Care Center. Both the Rinbutsuken Institute and the Sophia Grief Care Institute are organizations within Japan that have recently started cultivating such caregiver guides, which in the professional world are often called “chaplains”. Working from different religious standpoints but in cooperative settings, these two organizations are confronting the various forms of suffering now prevalent in Japan, such as depression, suicide, disaster trauma, the death of so many elderly, and all the grief that accompanies these issues.
While the Rinbutsuken Institute and the Sophia Grief Care Institute have been collaborating across religious lines for a few years, this symposium was a landmark event in the collaboration between medical and religious worlds in Japan. The modern medical world has largely dismissed the role of religious professionals in the care of patients, although the practice of “team care” with certified, professional chaplains has become somewhat standard in the United States. Since the end of World War II, Japan has been a resolutely secular state and has constitutionally barred the role of religious professionals in public sector work. This symposium was the first time a top level medical school, such as the Jikei School of Medicine, has collaborated with religious based organizations for a public event on the ways to collaborate for better patient care.
The host of the symposium was Prof. Dr. Naohito Shimoyama, Head of the Department of Palliative Medicine at Tokyo Jikei Medical University. Along with his wife and co-collaborator, Prof. Dr. Emi Shimoyama, they have recently brought in the Director of the Rinbutsuken Institute, Rev. Hitoshi Jin, and his colleague, Rev. Gakugen Yoshimizu, to serve as spiritual care workers and Buddhist chaplains at the hospital. A third collaborative partner was Prof. Susumu Shimazono, who was a leading scholar on contemporary religion at Tokyo University and is now the Director of Sophia’s Grief Care Institute while also serving on the Board of Directors for Rinbutsuken. These collaborative connections across independent organizations were until recently extremely difficult to cultivate in Japan, but are now breaking new ground for the future of holistic care, both medical and spiritual.
Presentations on Going Beyond Mindfulness Practice for Being with Suffering & Grief
To galvanize such collaboration, the Rinbutusken Institute with its international networks brought in three caregiver guides or “chaplains” from different parts of the world for this one-day symposium: Prof. Elaine Yuen, Associate Professor and Chair of the Department of Wisdom Traditions at Naropa University in the United States; Rev. Gustav Ericsson, a Christian priest in the Lutheran Church of Sweden with Japanese Soto Zen ordination; and Ven. Kuppiyawatte Bodhananda Thero, the founder and the Director of the Mithuru Mithuro Movement, the first and the largest Buddhist drug rehabilitation center in Sri Lanka. These three speakers are all using a range of contemplative practices that include mindfulness to be with the suffering of the traumatized. However, they brought to the audience a much wider understanding of mindfulness as not just a breathing technique for stress reduction but also as a method which combined with other forms of spirituality can develop numerous pro-social qualities for caring for others and transforming institutions.

Prof. Yuen began the symposium by immediately introducing a different seminal concept in Buddhism than mindfulness, that is compassion (karuna). She noted that healthcare is by nature centered around interpersonal connection, because at its root an awareness of and feeling for the pain and suffering of others impels and empowers people to not only acknowledge but also act. This is the essence of compassion. However, in such intensive environments like hospitals where there is so much suffering, something called “compassion fatigue” often occurs. This is a stress response from caring without expected rewards, results, and often closure that results in a diminished capacity for empathy and interpersonal engagement. Such “compassion fatigue” manifests in a variety of issues for caregivers, such as burnout from cumulative work, demands, and stress; secondary trauma from the dysfunction that arises from prolonged exposure to the suffering of others; moral distress from conflicts when a clinician knows what is right but cannot do it; horizontal hostility from disrespect among members of their professional peer group; and the structural violence inherent in many modern medical institutions which amongst other things must balance profit with care.
To meet these problems, she explained, mindfulness practice for the caregiver has become an increasingly important and popular practice in the United States. This shift has occurred from the mounting research evidence of its effects on emotional regulation and improved attention, greater calm and stress reduction, and enhanced coping skills. However, Prof. Yuen and other Buddhists in the field are now trying to integrate other Buddhist based contemplative strategies, such as “self-compassion”. Drawing on a variety of Buddhist teachings—especially the Four Divine Abodes (brahma-vihara) of loving-kindness (metta), compassion (karuna), sympathetic joy (mudita), and equanimity (upekkha)—American Buddhists in clinical and hospital environments are attempting to practice and transmit practices to develop warmth and understanding in oneself in times of professional suffering, failing, and feeling inadequate. Prof. Yuen explained that this involves practices to develop empathy and the ability to regulate one’s own arousal to situations so that one develops resilience rather than becoming overwhelmed. There is also the practice of perspective taking to develop congruence in goals and values between fellow clinicians and patients and their families. The practice of moral sensitivity is another important key in being able to recognize conflicts and obligations within the institution and to support caregiver decision-making. In this way, Prof. Yuen outlined the ways the holistic Buddhist approach of ethics (sila), meditation (samadhi), and causal insight (panna) work together to support a caregiver in navigating the wide variety of issues that arise in working in healthcare organizations.
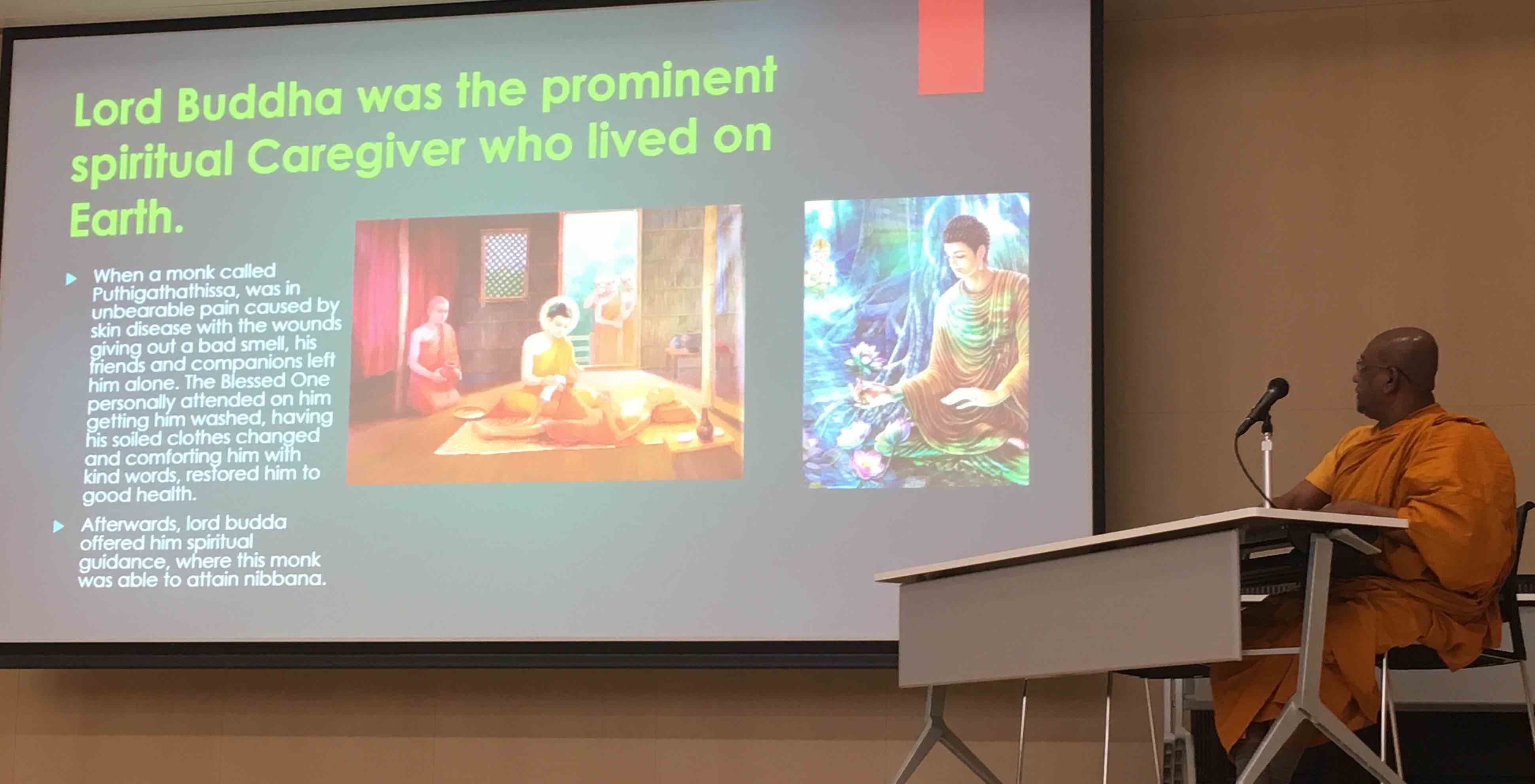
Ven. Bodhananda from Sri Lanka took the audience into a deeper understanding this key practice of the Four Divine Abodes, which are so critical in developing the skills that Prof. Yuen discussed. Ven. Bhodhananda’s work has not been in the kinds of public healthcare facilities that Prof Yuen outlined but in his own drug rehabilitation center for young men that he established in 1987. The name of the organization, Mithuru Mithuro, means “compassionate friend”, and the unique aspect of his center is the creation of a family system rather than a professionalized institution. All senior staff and counselors at the center were former patients themselves, creating a shared intimacy and respect among first time addicts and fully rehabilitated elder brothers. In explaining the process of their center, Ven. Bodhananda noted that if one is willing to work with suffering in order to help others to relieve their pain, first they must strengthen their own personalities by developing the basic human qualities according to the Buddha’s teachings of loving-kindness, compassion, sympathetic joy, and equanimity. He explained that these practices help to level social barriers, build harmonious communities, revive joy and hope long abandoned, and promote human brotherhood against the forces of egotism. In a therapeutic community, he has found these are very important to enhance treatment.
Ven. Bodhanana then explained the actual practice of meditation on these four “sublime states”, a practice that is as common in world of orthodox Buddhism as is basic mindfulness practice. For an example, he explained, we might select loving kindness as the specific subject of meditation. First, we start with an aspiration for our own wellbeing, using it as a point of reference. Then we gradually extend it to other beings by starting with someone we have loving respect for, like our parents or a teacher, then to dearly beloved people, to indifferent ones, and finally to enemies, if any, or those disliked. Persistent meditative practice of this method, he explained, will make these four qualities sink deep into the heart so that they become spontaneous attitudes. This practice will systematically break down conflicts we have with others, and we will be able to be more sensitive towards their suffering.
Ven. Bodhananda concluded by saying that the rehabilitation process followed by Mithuru Mithuro is not only for drug addicts. Anyone is who is suffering, as well as caregivers who are expected to offer support, can follow this process in order to develop these sublime states in themselves. He emphasized that we cannot categorize the distressed into a permanent group, because we all have the tendency to face similar addictions in our lives. We all are in same boat, so all are subject to addiction if we are not developing our spirituality. In this way, Ven. Bodhananda’s vision is not limited to using mindfulness and other Buddhist practices to develop coping mechanisms but is rather much vaster to include the fundamental transformation of each individual. Having rehabilitated over 5,000 addicts since 1987, Ven. Bodhananda center has been transforming young men into true leaders in society, who have been able to go forth and offer guidance and support to others in sorrow or fear, in stress or trauma.
Rev. Gustav Ericsson also brought a deeper and more nuanced understanding of meditative mindfulness in his talk. Before becoming a priest in the Lutheran Church of Sweden in 2010, Rev. Ericsson began his spiritual journey studying and practicing Japanese Zen in mid 1990’s and then receiving Dharma transmission from the Soto Zen teacher Gudo Nishijima Roshi in 2004. After being ordained as a Christian priest, he has served as a hospital chaplain at the regional University Hospital of Umea in northern Sweden and at a hospice for palliative care. He has also served as a counseling priest with the Lutheran Church’s national suicide prevention hotline, which has a national emergency number as well as chat rooms and mailbox online.
Rev. Ericsson explained that the key principles of his chaplaincy—being aware of his inner prayer room, walking slowly, entering a room with empty hands, seeing the Christ that is already here, and releasing the weight—are all to a large extent upheld and nourished by his practice of sitting and walking meditation. He noted that the sitting and walking of Zen meditation has become one with his service as a Christian hospital priest. He then explained how Buddhist mindfulness training has served as a platform for incorporating a variety of deeper practices. When he started working at the hospital, one of the first things his religious colleagues invited him to do was to practice embodying himself as a prayer room. For him, this is an image of how to be present in hospital rooms, corridors, and wards as a sitting and walking prayer room, which means providing an open and welcoming space that has many possibilities.
Another important practice for Rev. Ericsson is to enter every room with empty hands. This means letting go of ambitions and ideas about what to say, do, and accomplish. Rev. Ericsson explained that he tries to empty himself in order to be able to receive the people and the situation that he meets in the room and to enter with open questions and a willingness to listen and learn how he can be of service. For him, this practice of entering a room with empty hands does not mean that he denies his training, experience, and knowledge. Rather, he noted that in the moment of touching the handle and opening the door, he practices letting go of ambitions, tools, and fixed ideas while trusting in something bigger than his own thoughts and something greater than his little self. Rev. Ericsson insights here—the emptying of the self so that one can be “enlightened” by others forms[1]—embody the essential Buddhist wisdom (panna) that comes about from a deeper meditative insight (vipassana) attained beyond the basic calming and de-stressing (shamatha) of mindfulness practice.
Panel Discussion and Conclusion
After the conclusion of these presentations, Dr. Shimoyama, Rev. Jin, and Prof. Takaki Ito offered some short comments and then questions which led to a wide ranging two hour discussion. One of the most important issues that arose was the continued struggle to harmonize and coordinate the disparate approaches towards care of the medical and religious worlds. Prof. Ito of the Graduate School of Applied Religious Studies at Sophia University noted that the medical model focuses on objectivity and rationality in a diagnostic analysis. However, today’s speakers did not speak of a linear cause and effect model, but more of a dialectical model involving an interaction or relationship between patient and caregiver that includes subjective modalities like hope, the meaning of life, and values. While Prof. Ito said that he is sympathetic to these approaches, he noted that in Japan, as opposed to many other countries, there is absolutely no dialogue around spiritual or contemplative care in the medical world. In this way, he feels the need for some sort of data or evidence of these spiritual care methods to gain a foothold in Japanese medical institutions to be able to begin this work.

Prof Yuen responded that in the United States there is increasing research on the impact of chaplaincy, especially in terms of the financial bottom line of hospitals and their need to save/make money and to increase consumer satisfaction. Rev. Jin and his colleague at Rinbutsuken, Jonathan Watts, learned about this work on their visit to John’s Hopkins Hospital, which has a number of quantitative research studies on the effects of chaplaincy services. Rev. Ericsson noted that his hospital in Sweden developed a customer satisfaction survey with about 50% of positive results coming from how patients and family were received and handled, a role in which chaplains can be an important part. Prof. Yuen cautioned, however, that the work of the chaplain and their positive effect is often in special encounters when a meaningful contact or communication is made, like a sacred moment. This is very hard to do a quantitative analysis of and develop a predictive model for, even though its effect is well understood. Rev. Ericsson concurred that it is clear that there are special spiritual moments for the dying and their families, but that it is problematic to try to measure, quantify, or pre-arrange.
In response to this extended dialogue, Dr. Shimoyama provided the closing remarks for this groundbreaking symposium. He admitted that medical people have been very resistant to the religious world, but added that there is much in medicine and palliative care that cannot be explained by science. He reflected that sometimes when he is with a patient, he just wants to run away because the suffering is so severe. There are problems like this that cannot be solved by science, and religious people can help fill in these gaps. Thankfully, he was made aware of these issues by the late Dr./Rev. Masahiro Tanaka—a graduate of Jikei University and a Shingon Buddhist priest who ran a hospital and care home from his own temple in Tochigi. Rev. Tanaka’s temple has served as a training center for chaplains-in-training from the Rinbutsuken Institute, and it was Rev. Tanaka who introduced Rev. Jin to Dr. Shimoyama and Jikei University Hospital. Dr. Shimoyama concluded that he now feels very proud to be working with religious people. The important thing is to realize what we are lacking and to aim higher. We cannot accomplish much on our own, but when we join together with others, we can achieve greater results. In this way, he hopes Jikei University can become a center for the advancement of this work. Re-iterating Prof. Shimazono’s final comments for greater cooperative work, the symposium closed with the feeling that a new beginning had taken place in Japan for the interface of medical and spiritual as well as contemplative care for “all beings in this world of suffering”.
This report was prepared by Jonathan Watts, Research Fellow at the Rinbutsuken Institute, Lecturer at the Sophia University Grief Care Institute, and Executive Board Member of the International Network of Engaged Buddhists (INEB).
[1] This recalls the famous words of the Japanese Soto Zen founder Dogen in his Genjo Koan: “To study oneself is to forget oneself. To forget oneself is to be enlightened by the ten thousand dharmas. To be enlightened by the ten thousand dharmas is to be freed from one’s body and mind and those of others.”
